
Every year, 15 million babies are born prematurely, that is more than 1 in 10 babies. Unfortunately, preterm birth complications are one of the leading causes of death among young children.
Among them, a small number of babies defy the odds and come way too early to the world at less than 25-28 weeks in gestation. These are considered “extremely premature births”.
Surviving the birth
Babies born so early are fragile and very underdeveloped. Their lungs lack the slippery surfactant that prevent airways from collapsing upon exhalation. To survive, the tiny newborns must be given a surfactant treatment.
In low-income settings, these extremely premature babies often die due to a lack of cost-effective care, including warmth, breastfeeding support and basic care for infections. However, in high-income countries, “miracles” occasionally hit news headlines.
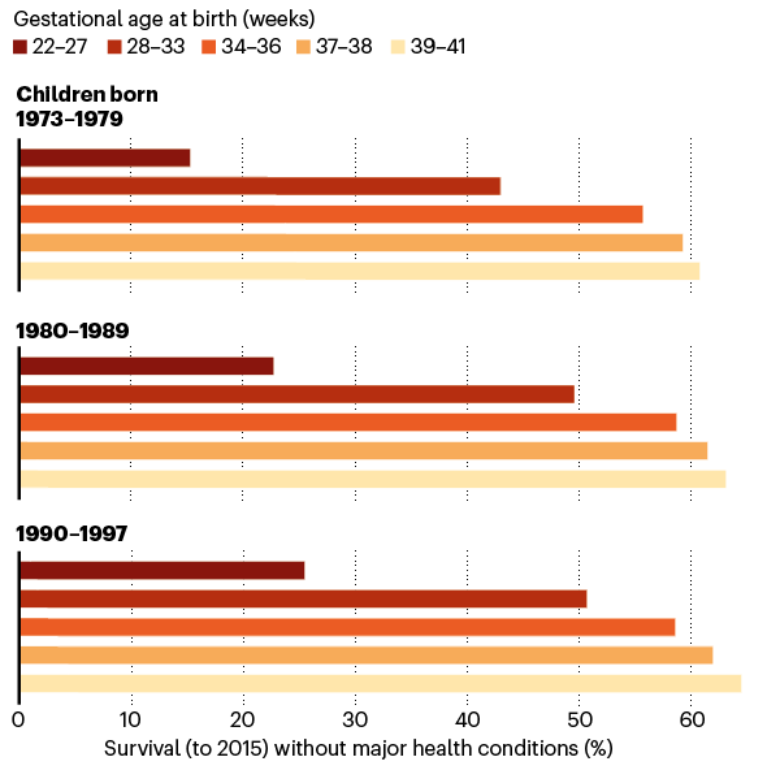
The late twentieth century marked an important time of breakthroughs for neonatal medicine. Very few preterm infants could survive in the past due to underdeveloped lungs. In the 1970s, Australia introduced ventilators, which helped but also caused lung injuries.
In the following decades, corticosteroids were introduced to mothers to help mature the baby’s lungs. However, the real game changer was the surfactant treatment that arrived in the early 1990s. It brought the death risk of premature infants to 60-73% of what it was before.
In a large Swedish cohort, we can see that the proportion of babies who live beyond 18 years old without medical conditions increased the most dramatically in the extremely premature groups by late 1990s.
source: Nature
Today, babies born as early as 22-24 weeks have a good chance of making it. In the UK, 35%. 38% and 60% of babies born at 22, 23, and 24 weeks survive, respectively.
More challenges to come
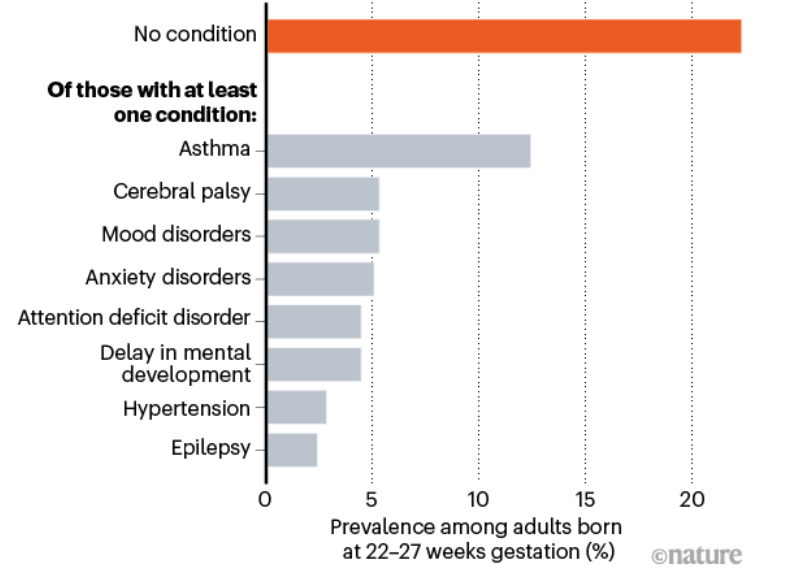
However, surviving birth is just their first challenge. These babies still face a long list of potential ongoing disabilities. More than three-quarters of the extremely premature babies had one chronic health condition by adulthood.
source: Nature
A report using data from the Swedish birth registry found that out of the 5,391 extremely preterm babies, 78% had at least one condition on the graph above compared to the 37% for full-term babies. 68% had predictors of early mortality, such as heart disease, which is almost a four-fold increase compared to full-term babies.
In another study from the United States, researchers found that 65% of the premature babies born at 23-24 weeks were ready to start kindergarten at the standard age, whereas 85.3% of the full-term babies were ready at the same age.
It seems that “miracle babies” have a tricky start in their life, but one study also suggested that their quality of life becomes comparable to others when reaching adolescence. As the earliest “miracle babies” enter adulthood and middle age, scientists are now looking at their long-term health sequences.
Long-term consequences of extremely premature birth
Camille Girard is a 27-year-old aspiring scientist working on the long-term consequences of being born extremely premature. She was born at just 26 weeks of gestation, when the doctors declared her “death” at the time. She has come a long way.
The biggest health concern for people like Camille is their lung function, which is also a key predictor of cardiovascular disease and death. Extremely premature babies were more likely to experience lung damage due to ventilators, inflammation and infection at birth. Although more research is needed, some respiratory physicians have noticed a new type of patients who experienced breathlessness in their 20s despite being non-smokers. These patients were born prematurely before 32 weeks of gestation, which may be linked to their symptoms.
In addition, researchers have noticed young adults who were born before 28 weeks at increased risk of high blood pressure. However, preliminary data from a pilot study of exercise intervention suggests that their heart functions may be improved with an active lifestyle.
What’s the future like?
As extremely premature birth survivors grow up, we have learned that their life is the most challenging in the first few years after birth. Numerous clinical trials are underway for assessing longer-term health consequences.
Researchers are also refining the care given to premature babies to minimise the damage of certain medications. for example, two growth factors called IGF1 and VEGF may be given to premature babies to protect their lungs and vision.
Apart from medications, social support is equally important. Parents are overwhelmed by feelings of quilt, fear and disappointment when they go home with premature babies, which could pave the way for parental depression and poorer care.
Some doctors are also advocating for preterm birth to be considered as a chronic condition that requires long-term follow up. At the moment, this cohort does not usually get special medical attention in adulthood, mostly because that doctors haven’t seen one of them yet.
In closing, there is no doubt that extremely premature babies and their family could expect many challenges. However, the future is not all doom and gloom with better neonatal care and understandings of long-term outcomes of premature birth.
Ovarian hyperstimulation syndrome (OHSS): How scary is it really?
Ovarian hyperstimulation syndrome (OHSS) is a well-recognised complication of IVF. The internet is also a source of scary anecdotes of OHSS and IVF trauma. What is it really like, should the risk of OHSS stop you from IVF?
What is OHSS?
Fertility drugs such as gonadotrophins are frequently used to stimulate the ovaries during IVF treatment to mature more than normal number of eggs per cycle. This allows the collection of more than one egg that can used to create embryos in the lab.
Why do we do it? Simple math. IVF is not a magic treatment that works 100% of the time, but the more eggs we have to try fertilisation, the more viable embryos we get. Since not all embryos survive implantation and become full-term babies, having a higher number from the get-go is crucial.
However, overstimulated ovaries enlarge due to multiple growing follicles. This can lead to fluid leaking into the belly, and in severe cases, into the space around the heart and lungs. Symptoms vary depending on the severity of OHSS:
- Mild OHSS: abdominal swelling, discomfort and nausea
- Moderate OHSS: worse swelling and discomfort, abdominal pain and vomiting
- Severe OHSS: extreme thirst and dehydration, small urine volume, tight chest, breathlessness, blood clots in the legs and lungs, abdominal pain, rare death
Usually, symptoms should resolve in 7-10 days. If the fertility treatment does not lead to a pregnancy, OHSS should disappear by the time of your next period. However, if you do become pregnant, OHSS may get worse and last for longer.
How many people actually get OHSS?
Just like anything scary, OHSS gets exaggerated by the media. Most cases of ovarian hyperstimulation are mild and can settle by themselves. The severe cases of OHSS that are often picked up by media are only the rare occasions.
in Australia, the percentage of assisted reproductive technologies resulting in hospital admission due to OHSS has dramatically reduced to less than 1% in 2018.
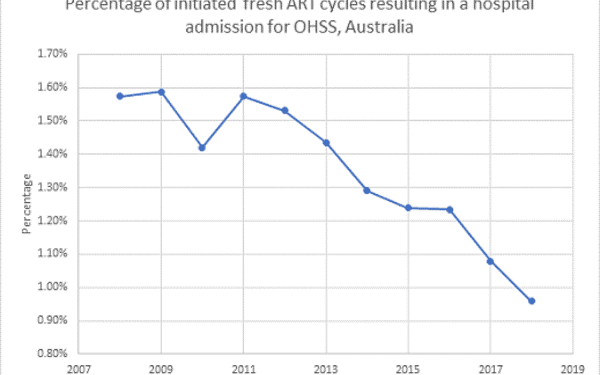
Source: IVF Australia
Who can get OHSS?
Despite severe cases being rare, mild OHSS is not uncommon in women undergoing IVF. The risk is higher in women who:
- have polycystic ovary syndrome (PCOS)
- are under 30 years old
- have had OHSS in the past
How to prevent or treat OHSS?
There are strategies that can lower the risk of OHSS. The most common one is to reduce the dose of ovarian stimulation medications. Your fertility specialist will be able to decide on the specific stimulation drug and dosage after assessing your condition.
Since pregnancy can make OHSS worse or last longer, it is recommended to avoid immediate pregnancy in the same cycle of egg collection. Instead, eggs or embryos can be frozen and transferred at a later cycle when no ovarian stimulation drugs are used. Researchers have found that freezing all embryos is beneficial for high responders (more eggs matured) in particular.
A key aspect of OHSS prevention is close monitoring of the symptoms. Routine office visits for ultrasound scans allow measurement of the ovaries and fluid. Your fertility specialist will be able to visually assess the extent of ovary enlargement during your IVF treatment.
If you already experience mild symptoms, there are a number of treatments that can help relieve symptoms, including:
- pain relief drugs, eg. paracetamol
- anti-sickness drugs
- procedures to drain fluid accumulation
If in rare cases, these treatments do not improve your symptoms, you may be admitted to the hospital for close monitoring.
Since your ovaries are enlarged and painful, avoiding strenuous exercise and sex are also recommended to avoid injury to the ovaries.
Important takeaways
Hopefully you now have a more complete view on OHSS. Although OHSS can be life-threatening, most cases are mild and can be prevented or managed. During your IVF cycle, you should pay close attention to any symptoms of OHSS and report them to your doctor. You will also likely get ultrasound scan check-ups that provide more information on your follicle development status.
But coming back to our original question, should you let the risk of OHSS stop you from trying IVF? Not really!
For more information, you can consult Melbourne-based fertility specialist Dr Alex Polyakov.